ACL Prehab: What “Ready for Surgery” Looks Like (and How to Get There Faster)
If you’re guiding an ACL patient toward reconstruction, prehab gives you leverage. We focus on knee status and a short set of measurable targets so you can keep progress steady into surgery and through the first phases of rehab.
Designed for clinicians managing ACL cases: Physiotherapists, DPT/PTs, Athletic Trainers, Rehab Managers, Lead Clinicians, and Rehab Directors.
What you’ll get on this page:
-
A simple “ready for surgery” checklist you can scan in under a minute
-
Prehab targets for ROM, effusion, quad activation, and strength
-
Programming ideas you can scale across settings and equipment availability
What the downloadable guide adds:
A complete phase-based framework with readiness criteria, progression logic, and return-to-sport checkpoints.

GET THE ACL REHAB GUIDE
Includes a phase-based progression, criteria checkpoints, and a practical testing checklist for clinic use.
Learn MoreWhy prehab changes the post-op course
Prehab helps you enter surgery with a knee that tolerates load and responds predictably to training. When you and your patient build capacity pre-op, you set cleaner expectations for the first weeks after reconstruction and you protect the early phase from avoidable setbacks.
Three outcomes we plan for during prehab:
-
A calmer knee you can train consistently
You and your patient can progress with fewer swings in swelling and symptoms, which makes weekly decisions clearer.
-
Reliable extension and better movement options
When extension is consistent, you can choose exercises and gait progressions with fewer compensations.
-
More usable quadriceps function on day one post-op:
Pre-op quad activation and strength work often carries forward. That gives you a better starting point for early loading, control, and confidence.
Next, we’ll outline the readiness indicators we use in clinic and the benchmarks that support a smoother transition into surgery and early rehab.
ACL prehab readiness: Green, Yellow, and Red indicators you can use today
We use a simple traffic-light check to guide decisions in the final stretch before surgery. It helps you align the plan with how the knee is behaving, and it gives your patient clear targets to work toward.
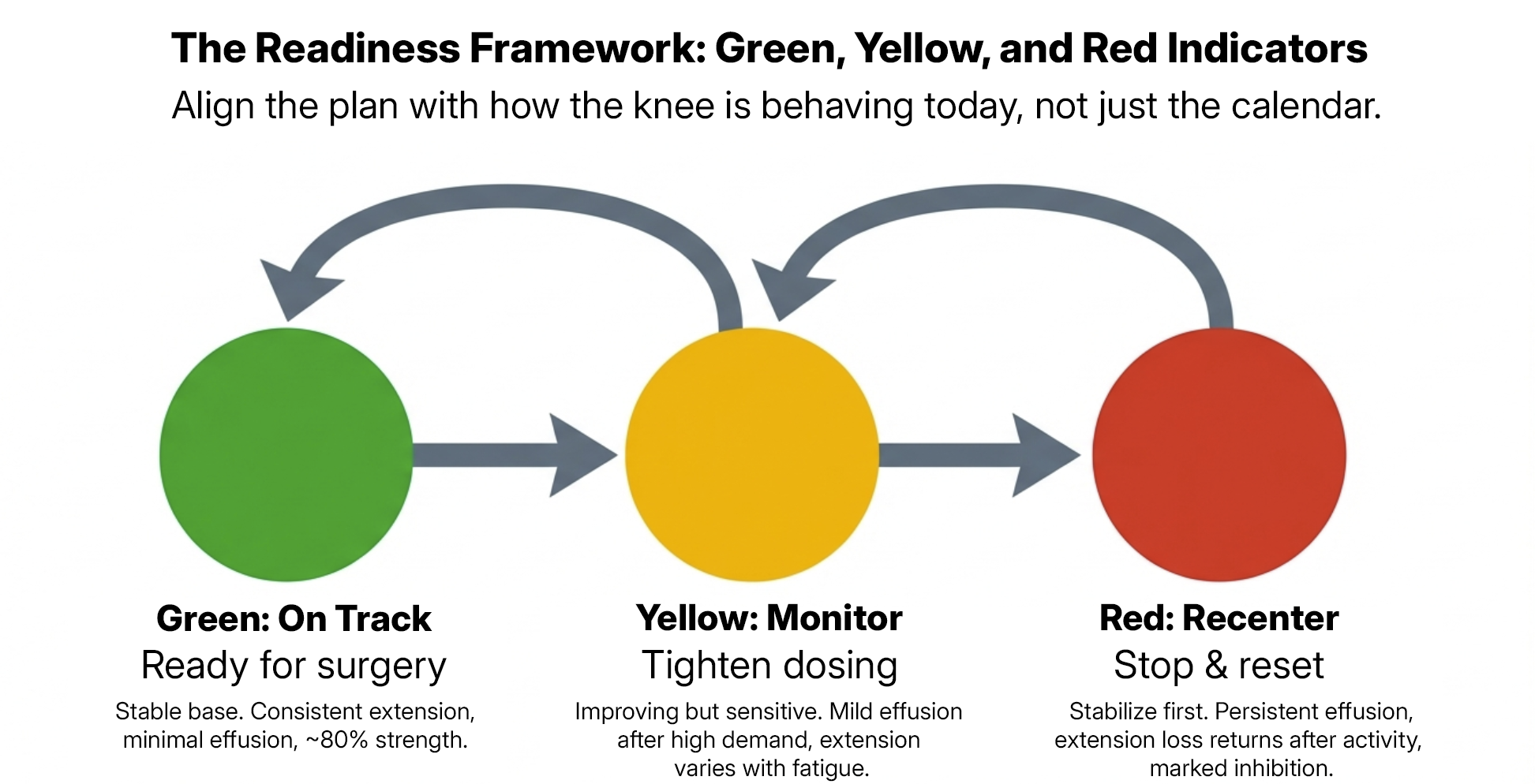
Green indicators (on track for surgery readiness)
Use these when you want a stable base going into reconstruction.
- Extension is full and consistent across days and after training sessions
- Effusion is minimal and predictable with your current loading plan
- Quadriceps activation is strong during basic tasks (no visible lag, clean terminal control)
- Strength trend is moving in the right direction and you can document progress week to week
- If you can measure it: a practical pre-op benchmark is ~80% quadriceps strength compared to the uninvolved limb (this is a useful target, not a hard requirement — timing of surgery, ongoing irritability, or limited pre-op window may make 80% symmetry unrealistic in some cases)
Yellow indicators (keep progressing with closer monitoring)
Use these when the knee is improving, and your plan needs tighter dosing.
- Mild effusion that increases after higher-demand days
- Extension varies with workload, travel, or time on feet
- Quadriceps control fades with fatigue or higher volumes
- Strength work feels limited by symptoms rather than effort tolerance
What we do in this zone: tighten the dose, protect extension, and keep the patient training with consistent week-to-week progress.
Red indicators (re-center before you push)
Use these when you need to stabilize the knee status before you chase higher outputs.
- Persistent or increasing effusion that lingers beyond the next day
- Extension loss that returns after training or normal daily activity
- Marked quadriceps inhibition that blocks clean control in simple tasks
- Strength is trending down despite appropriate dosing and adherence concerns are emerging
These indicators support clinical decision-making. Surgical timing and readiness remain a shared decision between you, the patient, and the surgical team.
Next, we’ll break down the non-negotiables we prioritize in prehab: extension, effusion control, and quadriceps activation.
The prehab non-negotiables: extension, effusion control, and quadriceps activation

When you’re preparing an ACL patient for reconstruction, we keep the focus tight. These three priorities influence how the knee behaves after surgery, how quickly you can load, and how confidently the patient moves through early rehab.
1) Extension: make it consistent, then protect it
We aim for restoration of the patient’s normal extension range that holds across the day and stays consistent after training. For some patients, that includes physiologic hyperextension seen on the uninvolved limb, when appropriate and consistent with surgical guidance.
What you look for in clinic
-
Extension symmetry side to side in a relaxed position, matching the uninvolved limb’s normal range
-
Clean terminal knee control during simple tasks (gait, step-down, quad set)
-
Extension that stays stable after longer days on feet
What we do to get there
-
Dose extension work daily in small, repeatable exposures
-
Pair extension work with quadriceps activation so the patient can “own” the range
-
Build training volume in a way the knee can tolerate without losing extension
Quick rule we use: if extension worsens after a session, reduce the next session’s dose and rebuild from a level the knee holds.
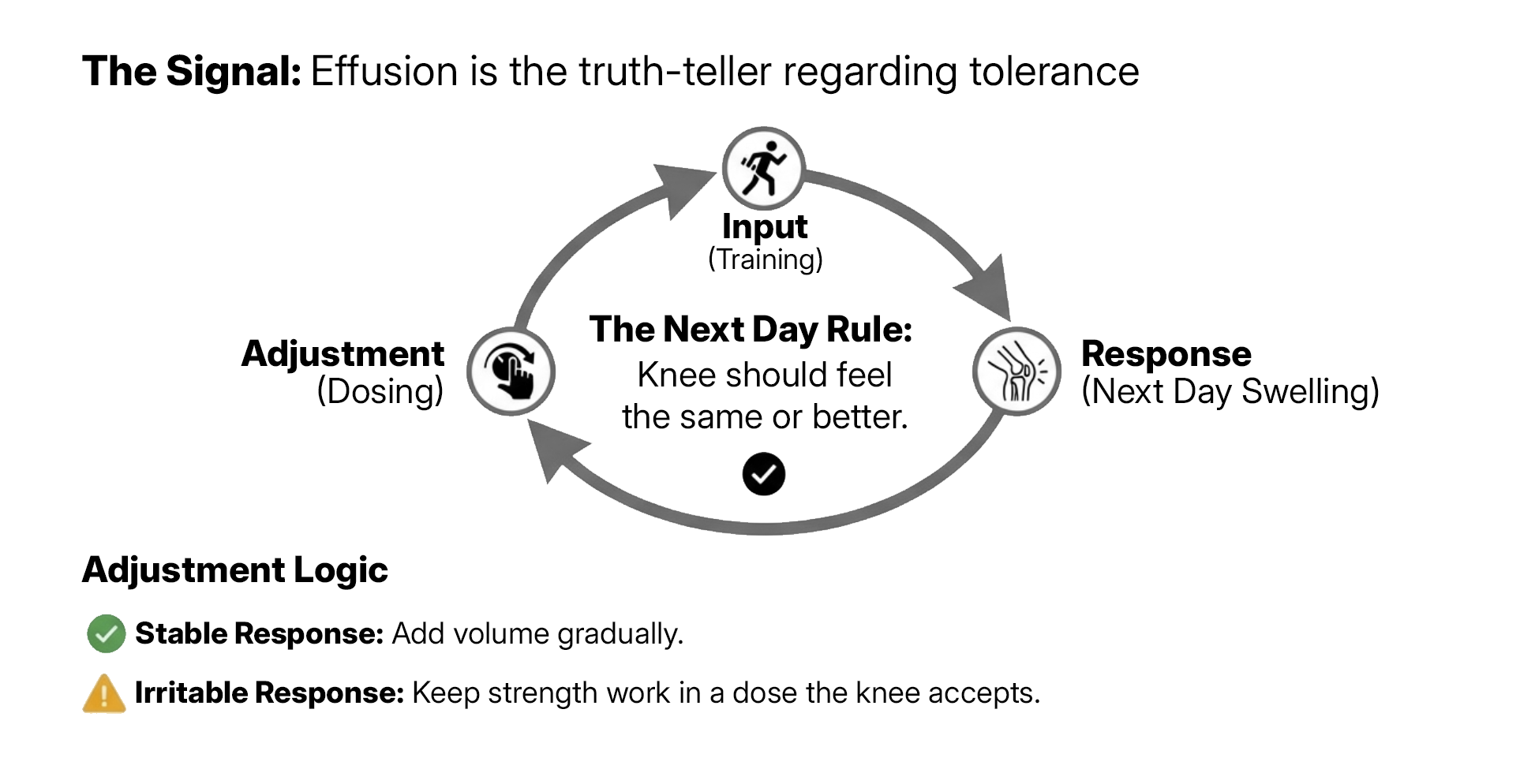
2) Effusion control: use the knee’s response to guide your dosing
Effusion tells you how well the knee is tolerating the plan. We use it as a daily signal to shape volume, intensity, and exercise selection.
What you look for
-
Effusion that stays minimal and consistent across the week
-
A clear “next-day response” to training that you and the patient can predict
-
Symptoms that settle with simple recovery inputs (sleep, compression, elevation, cycling or walking as tolerated)
How you adjust
-
Keep strength work in a dose the knee accepts, then add volume gradually
-
Choose exercise options that maintain movement quality and reduce irritability
-
Build aerobic work as a tool for circulation and tolerance when appropriate
Knee response check (simple): you want the knee to feel the same or better the next day. Use that feedback to guide progressions.
3) Quadriceps activation: earn clean control before you chase higher outputs
We want the quadriceps to contract strongly and consistently. Better activation supports extension, improves gait quality, and sets up your early post-op strengthening.
What “good” looks like
-
Strong quad set with visible contraction and minimal co-contraction patterns
-
Straight leg raise without lag (when appropriate for the patient)
-
Clean terminal knee control in basic closed-chain tasks
How we build it
-
Start with high-quality reps and frequent practice
-
Use short sets, full attention, and rest that keeps the contraction crisp
-
Progress to loaded work once control holds under fatigue and higher reps
With these non-negotiables in place, you can set strength targets that are measurable and realistic across different clinics and tools.
Pre-op strength targets you can measure and progress
Once extension, effusion, and quadriceps activation are stable, strength becomes the lever that drives better tolerance and cleaner early loading after reconstruction. We aim for targets you can explain to the patient and track across weeks.
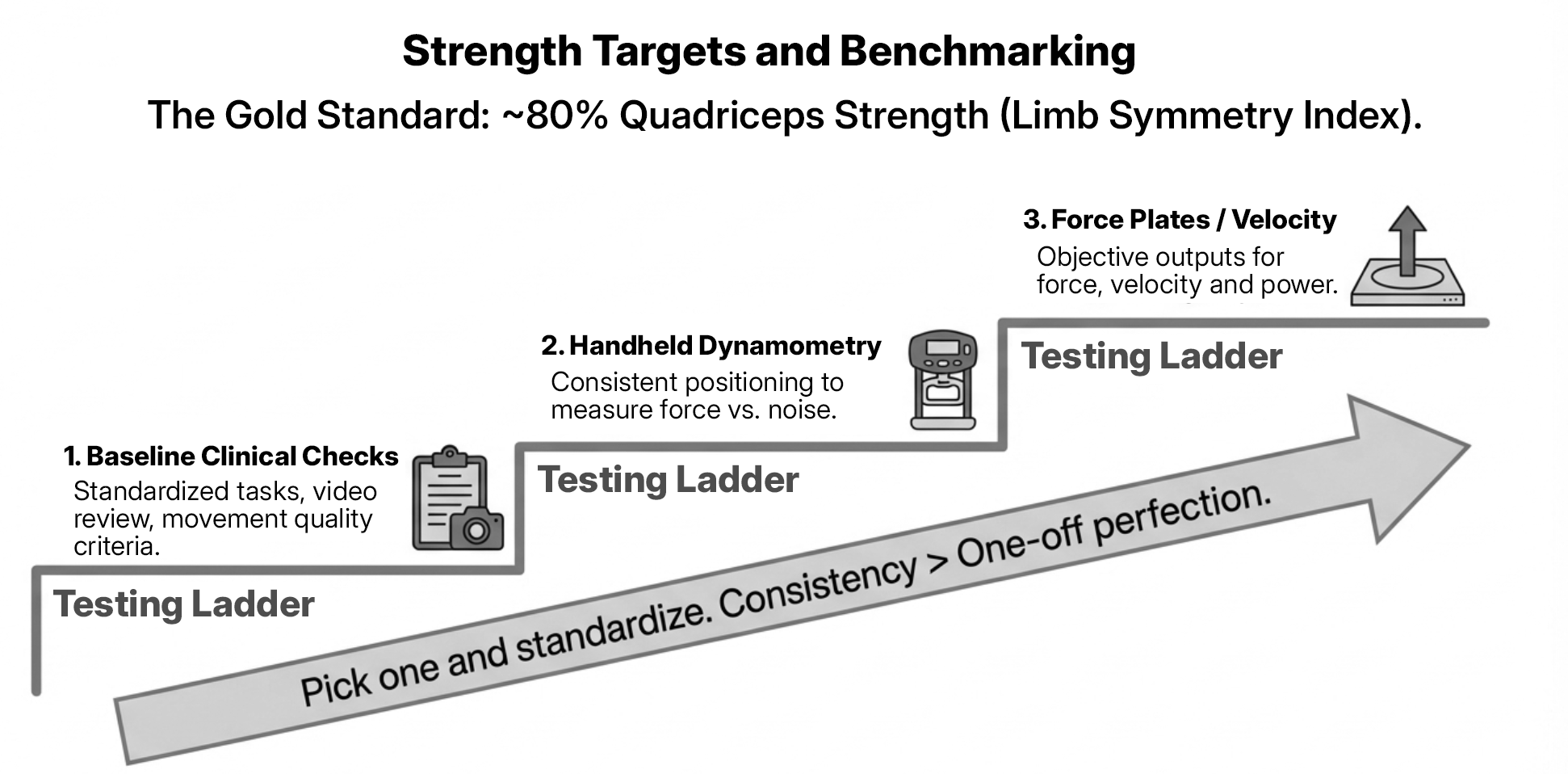
The benchmark we use when you can quantify quadriceps strength
A practical pre-op goal is ~80% quadriceps strength (a good target, but not always achievable, depending on timing of surgery and knee irritability) compared to the uninvolved limb. You can treat this as a readiness benchmark and a communication tool for expectations.
How we apply it
-
Track the trend weekly or every other week
-
Build the plan around progressive exposure the knee tolerates
-
Document symptoms alongside output so you can dose with confidence
A simple “testing ladder” you can implement in most settings
Choose one option you can repeat consistently. Consistency gives you better decisions than a one-off “perfect” test.
-
Baseline clinical checks (low equipment)
Use standardized tasks and clear criteria for movement quality, control, and fatigue. Record short video from the same angles to compare week to week.
-
Handheld dynamometry or fixed set-ups (low-cost objective)
If you have access, use a consistent position and stabilization strategy so changes reflect strength, not test noise.
-
Output-based strength and velocity measures (more instrumented)
If your facility uses tools that capture force, velocity, or power, you can add objective outputs that help you fine-tune loading and intent.
Pick one method and standardize it. Reliable repeat testing supports clearer clinical decisions and clearer patient messaging.
What you do when strength work irritates the knee
Effusion and extension remain the guardrails. When the knee response worsens, we adjust dose before we change direction.
-
Reduce total volume and keep intent high
-
Use ranges and exercise selections that maintain extension and control
-
Progress in small, repeatable steps that the knee tolerates
Next, we’ll share simple prehab templates you can scale for an irritable knee, capacity-building, and higher-function preparation.
Prehab templates you can run in 20 minutes
We keep prehab sessions simple and repeatable. Your goal is to train consistently, protect extension, and build quadriceps function without triggering an effusion spiral. Use these templates as starting points and scale the dose to the knee’s next-day response.
How to use these templates
- Pick one template per session based on knee status and recent response
- Keep movement quality high and stop sets when control degrades
- Progress one variable at a time (load, range, reps, or complexity)
- Re-check extension and effusion later the same day and the next day
Template A: Irritable knee (calm, move, activate)
Purpose: restore confidence in movement, protect extension, build quad recruitment
Session (20 minutes)
- Extension reset (3–5 min)
Low-load sustained extension work as tolerated, then a brief re-check. - Quad activation block (5–6 min)
- Quad sets: 3–5 sets of 5–8 high-quality reps
- Terminal control drill (band TKE or similar): 2–3 sets of 8–12
- Controlled strength exposure (6–8 min)
- Sit-to-stand or supported squat pattern: 2–3 sets of 6–10
- Step-up (low height) or split-stance isometric: 2–3 sets of 15–30 sec holds
- Easy aerobic flush (3–5 min)
Bike or brisk walk as tolerated.
Knee response check: you want effusion stable and extension unchanged the next day. If the knee reacts, reduce volume first.
Template B: Capacity-building (progress strength with stable knee status)
Purpose: build quad strength and single-leg capacity while keeping symptoms predictable
Session (20 minutes)
- Prep (2–3 min)
Bike or marching warm-up plus a quick extension check. - Primary strength (8–10 min)
- Leg press or squat pattern in tolerated range: 3 sets of 6–8
- Split squat or rear-foot elevated split squat (as tolerated): 2–3 sets of 6–8 each side
- Single-leg control (5–6 min)
- Step-down or lateral step-down: 2–3 sets of 6–10
- Hip hinge pattern (RDL variation): 2 sets of 6–10
- Finish (2–3 min)
Light conditioning or calf work if appropriate.
Progression rule: increase load or reps when the knee response stays predictable for two sessions in a row.
Template C: Higher function prep (strength plus controlled deceleration)
Purpose: keep strength progressing and introduce controlled landing/braking mechanics.
Note: This level of exposure depends on knee status, timing to surgery, and clinician judgment. Not all pre-op patients will tolerate or require deceleration or landing work.
Session (20 minutes)
- Prep (2–3 min)
Dynamic warm-up plus extension check. - Strength anchor (7–8 min)
- Squat or leg press pattern: 3 sets of 4–6
- Knee-dominant single-leg pattern (split squat or step-up): 2–3 sets of 5–8
- Deceleration mechanics (6–7 min)
- Controlled step-and-stick (forward or lateral): 3 sets of 3–5 each side
- Low amplitude landing to stable hold (as appropriate): 2–3 sets of 3–5
- Cool down (2–3 min)
Easy bike or walk.
Quality standard: you want quiet landings, stable trunk, and consistent knee position across reps.
Next, we’ll cover the red flags we watch for in prehab and what they often predict after surgery.
Prehab red flags that often slow early progress
Most prehab plans succeed when the knee stays calm, extension holds, and quadriceps function improves week to week. When progress feels sticky, a few common patterns tend to show up. We use these as clinical signals to tighten the plan and align expectations with the patient and surgical team.
Red flag 1: Effusion that stays elevated or climbs with training
If effusion lingers into the next day or trends upward across the week, it often limits quadriceps recruitment and reduces tolerance for progression.
What you can do
- Reduce total volume and keep the session dose repeatable
- Progress in smaller steps and re-check next-day response
- Use simple recovery inputs that the patient can execute consistently
Red flag 2: Extension that varies across days
Extension that comes and goes often predicts early post-op frustration. It can change gait mechanics, alter loading choices, and slow progress in basic strengthening.
What you can do
- Build a daily extension routine the patient can follow
- Re-check extension after higher-demand days
- Pair extension work with quadriceps activation so the patient owns end-range control
Red flag 3: Persistent quadriceps inhibition
When the quadriceps fail to “show up” reliably, you lose your anchor for early loading, gait quality, and confidence in simple tasks.
What you can do
- Use frequent, high-quality activation exposures
- Keep sets short and crisp, and stop when control degrades
- Choose strengthening options that keep symptoms predictable and movement clean
Red flag 4: Strength trend stalls or regresses
A flat strength curve often points to a dosing problem, poor recovery capacity, inconsistent adherence, or a knee that needs more stability in symptoms before you add load.
What you can do
- Standardize your testing method and re-check it for noise
- Adjust one variable at a time (volume, range, load, frequency)
- Confirm the home plan is realistic and that the patient can execute it
Red flag 5: Low readiness for the rehab process itself
Some barriers sit outside the knee. A patient’s schedule, support system, and confidence influence adherence and outcome.
What you can do
- Set a simple weekly plan the patient can follow
- Agree on one or two metrics you both track
- Use clear language around expectations for the first few weeks after surgery
If you want the full phase-based progression and the readiness checkpoints that connect prehab to early rehab and return-to-sport preparation, the downloadable guide lays it out step by step.

Want the full progression, criteria, and testing checklist?
This page gives you the key prehab priorities and practical targets for “ready for surgery.” The downloadable guide includes the complete phase-by-phase progression, readiness criteria you can document, and testing considerations you can apply across settings.
What you’ll get in the guide
- A phase-based ACL rehab framework from early rehab through return-to-sport preparation
- Criteria checkpoints for ROM, effusion, quadriceps function, strength, and capacity
- Practical testing options and a minimum-viable checklist for clinic use
- Common sticking points and troubleshooting cues clinicians can use
GET THE ACL REHAB GUIDE
Includes a phase-based progression, criteria checkpoints, and a practical testing checklist for clinic use.
Learn More
ACL prehab FAQs clinicians ask
1) What are the main goals of ACL prehab?
We use prehab to normalize knee status and build usable quadriceps function before reconstruction. In practical terms, you’re aiming for consistent extension, controlled effusion, reliable quad activation, and a strength trend you can document.
2) What ROM should a patient have before ACL reconstruction?
We look for restoration of the patient’s normal extension — including hyperextension if present on the uninvolved side and appropriate per surgical guidance — that stays consistent across the day and after training. Flexion matters as well, and extension usually drives early function and exercise tolerance.
3) How strong should the quadriceps be before surgery?
When you can quantify it, a practical benchmark is around 80% quadriceps strength compared to the uninvolved limb. You can use this as a readiness target and a way to set expectations for early post-op loading.
4) What if I can’t measure quadriceps strength objectively?
Pick one repeatable method and standardize it. Many clinics use a combination of consistent functional tasks, video review, and a structured progression of loading. If you have access to handheld dynamometry or fixed setups, you can add objective testing with minimal complexity.
5) How do you dose prehab when effusion increases after sessions?
We use the knee’s next-day response to guide dosing. When effusion climbs or lingers, reduce total volume first and keep the plan repeatable. Maintain extension work and quadriceps activation, then rebuild load in small, stable steps.
6) How often should a patient do prehab before surgery?
Frequency depends on knee irritability, access, and the patient’s schedule. We typically aim for consistent exposures across the week with a dose the knee tolerates, then progress gradually as the response stays predictable.
If you want the full phase-based plan and the readiness checkpoints that connect prehab to early rehab and return-to-sport preparation, download the ACL Rehab Guide.
About the Author
 Manoj “Manny” Patel is a Consultant Chartered Physiotherapist for Keiser UK & Ireland and a Chartered Physiotherapist (MSc, BSc (Hons), DiP, MSCP, SRP). He has over two decades of experience across physiotherapy, health, and fitness, with clinical and performance experience spanning the NHS, military settings, sport, and private practice.
Manoj “Manny” Patel is a Consultant Chartered Physiotherapist for Keiser UK & Ireland and a Chartered Physiotherapist (MSc, BSc (Hons), DiP, MSCP, SRP). He has over two decades of experience across physiotherapy, health, and fitness, with clinical and performance experience spanning the NHS, military settings, sport, and private practice.
This article was adapted from Manny’s ACL Rehab practitioner guide.
© 2026 Keiser Corporation | 2470 S. Cherry Ave | Fresno CA 93706